A Detailed Look At Laryngoscopy
What is laryngoscopy?
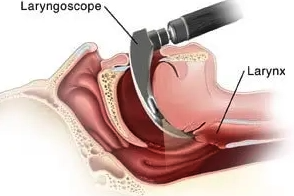
Laryngoscopy is an examination that allows your doctor to take a close look at your throat and larynx. Another name for larynx is the voice box. It lies on top of your trachea (windpipe).
The health of your larynx is very important because it holds your vocal cords, also called vocal folds. When air passes through your larynx and vocal cords, the cords vibrate and this results in sound production. This is what enables you to speak.
A laryngoscopy is performed by an “ear, nose, and throat” (ENT) doctor like the physicians at Potomac ENT. During laryngoscopy, the ENT doctor will put a laryngoscope in your mouth, or a mirror in your throat. In some cases, they insert both.
When is a laryngoscopy necessary?
A laryngoscopy helps your doctor to learn more about your condition. Of course, these are conditions that affect your throat. They include:
- Cough that produces blood
- Persistent cough
- Pains in your throat
- Hoarseness
- Bad breath
- Persistent earache
- Difficulty swallowing
- A growth in your throat
With a laryngoscopy, your ENT can extract any foreign object that is lodged in your throat.
How to prepare for a laryngoscopy
You should arrange for someone to drive you to and from the medical center. You may find it hard to drive for a couple of hours after anesthesia.
You may want to discuss with your doctor about the procedure. They will inform you of the necessary preparations to make. Depending on the type of anesthesia the doctor advises, you may need to stop eating for at least 8 hours before the procedure.
If you are currently on any medication, inform your doctor. Sometimes, you may be asked to stop taking the medications for at least a week before the procedure. Your doctor will let you know whether it is safe to continue or discontinue any prescribed medication.
What happens during the procedure?
You may be asked to undergo some tests just before the procedure. The results of these tests will help your doctor to have a better understanding of your symptoms. Tests usually ordered include:
- A physical examination
- CT scan
- Chest X-ray
- Barium swallow
In the case of the barium swallow, you will do an x-ray after the swallow. Barium is a contrast material that allows your doctor to have a clearer view of your throat. It is not poisonous and will be flushed out of your system within a few hours of swallowing it.
Laryngoscopy may take at least 5 minutes, and in some cases, up to 45 minutes. We have two types of laryngoscopies: direct and indirect.
Indirect laryngoscopy
An indirect laryngoscopy requires sitting straight in a high back chair. The doctor will then apply a local anesthetic or a numbing medicine on your throat. Your tongue will be covered with gauze and held to prevent it from blocking their view.
A mirror will then be inserted into your throat while your ENT explores the area. You may be asked to make a sound. The sound will cause your larynx to move. If there’s any foreign object lodged in your throat, your doctor will take it out.
Direct laryngoscopy
This is usually done in a doctor’s office or a hospital. You will be sedated, and won’t feel anything while the test is ongoing.
The doctor will insert a small flexible telescope in your mouth and slide it down your throat. Your doctor will then view your larynx closely through the scope. He can take biopsy samples and extract foreign objects or growths.
How are the results interpreted?
Your doctor may remove overgrowths, collect specimens, or extract foreign objects during a laryngoscopy. They may also take a biopsy. Your doctor will discuss your results and advise you on treatment options after the procedure based on the findings.
Article Resources
Joshi R, Hypes CD, Greenberg J, et al.: Difficult Airway Characteristics Associated with First-Attempt Failure at Intubation Using Video Laryngoscopy in the Intensive Care Unit. Ann Am Thorac Soc. 2017;14(3):368–75. 10.1513/AnnalsATS.201606-472OC
Retrieved from: https://pubmed.ncbi.nlm.nih.gov/27983871/
Wallace CD, Foulds LT, McLeod GA, et al.: A comparison of the ease of tracheal intubation using a McGrath MAC ® laryngoscope and a standard Macintosh laryngoscope. Anaesthesia. 2015;70(11):1281–5. 10.1111/anae.13209
Retrieved from: https://pubmed.ncbi.nlm.nih.gov/26336853/
Kleine-Brueggeney M, Greif R, Schoettker P, et al.: Evaluation of six video laryngoscopes in 720 patients with a simulated difficult airway: a multicentre randomized controlled trial. Br J Anaesth. 2016;116(5):670–9. 10.1093/bja/aew058
Retrieved from: https://pubmed.ncbi.nlm.nih.gov/27106971/
Mosier JM, Sakles JC, Stolz U, et al.: Neuromuscular blockade improves first-attempt success for intubation in the intensive care unit. A propensity-matched analysis. Ann Am Thorac Soc. 2015;12(5):734–41. 10.1513/AnnalsATS.201411-517OC
Retrieved from: https://pubmed.ncbi.nlm.nih.gov/25719512/
Subjects
Tags
Allergy Apnea Asthma balloon sinuplasty bronchitis CAdENT Chronic Congestion Deviated Septum Doctor Ear Nose Throat Ear Ringing ENT ent doctor ENT Doctor ent surgery Headaches Hearing Test Infection Laryngoscopy larynx Nasal Nasal Valve Collapse Nosebleed Potomac ENT Rhinosinusitis Sinus Sinusitis Sleep Sleep Apnea Snoring Surgery Therapy Throat Tinnitus TMJPeople Say
Great experience. They are courteous and knowledgeable.
Lisa Berry
Patient

Northern VA Office
14000 Crown Ct
Suite 201
Woodbridge, VA 22193
Call: (703) 499-8787
Northern VA Office
385 Garrisonville Rd
Ste. 208-209
Stafford, VA 22554
Call: (703) 499-8787
Northern VA Office
14000 Crown Ct
Suite 201
Woodbridge, VA 22193
Call: (703) 499-8787
Northern VA Office
385 Garrisonville Rd
Ste. 208-209
Stafford, VA 22554
Call: (703) 499-8787
© Copyright 2023 Potomac Otolaryngology, The Centers For Advanced ENT Care, LLC. All rights reserved. Empowered with arPlatform + arTeam.
© © Copyright 2023 Potomac Otolaryngology, The Centers For Advanced ENT Care, LLC. All rights reserved.
Empowered with arPlatform + arTeam.